Structure of Human Astrovirus
- Human astrovirus (virus causing gastroenteritis in humans) falls under Astroviridae (virus family) and genus Mamastrovirus (mammalian astrovirus genus).
- The particles (virus virions) are round in shape, 28 nm in diameter, with a smooth margin, displaying a five- or six-pointed star motif (star-like surface feature). The term astrovirus (Greek: astron–star) was coined to refer to this feature.
- They are non-enveloped, spherical, with a capsid (protein shell) of about 35 nm, icosahedral symmetry (20-faced geometric structure), and comprise single-stranded RNA with positive polarity (ssRNA(+), genome acts as mRNA).
- Surface projections (capsid spikes) are small, making the surface appear rough, spikes protruding from the 30 vertices.
- The capsid precursor protein (180 copies per particle) undergoes C-terminal cleavages (protein cut at C-terminal end) by host caspases (host proteases) during virus maturation. Infectious particles are generated by further cleavages of VP70 (capsid polyprotein) by extracellular proteases, resulting in three structural proteins.
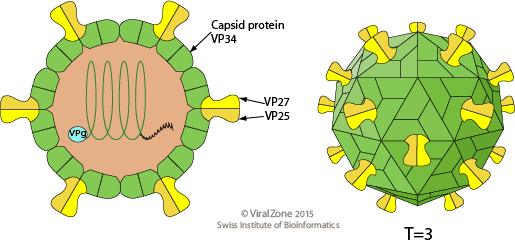
- VP34 (capsid shell protein) is derived from the highly conserved N-terminal region of the polyprotein and builds up the capsid shell, while VP27 and VP25 (spike proteins) are both derived from the variable C-terminal domain with different N termini and form the dimeric spikes.
- Buoyant density (density in solution) of the virions is between 1.35 and 1.37 g/ml in CsCl (cesium chloride gradient).
- There are at least 8 distinct serotypes (HAstV 1–8) (antigenic types) of human astrovirus, defined both antigenically and by genetic sequence differences.
Genome of Human Astrovirus
- The genome is monopartite, linear ssRNA(+) (single-stranded RNA with positive sense) of 6.8–7 kb in size. The 5′-terminus is linked to a VPg protein (viral protein genome-linked), and the 3′-terminus has a poly(A) tract (polyadenylated tail).
- The virion RNA is infectious and serves as both the genome and viral messenger RNA (acts as template for translation).
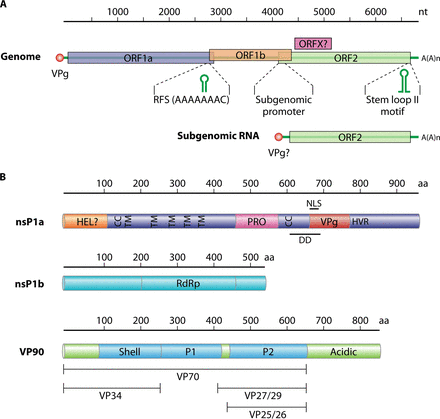
- The genome contains three overlapping open reading frames (ORF1a, ORF1b, and ORF2) (protein-coding regions).
- Nonstructural proteins (proteins not part of capsid) are translated from the genomic RNA as two large polyproteins, nsP1a and nsP1a/1b, through translational ribosomal frameshifting (shift in reading frame during translation).
- ORF1a and ORF1b encode the viral protease (protein-cutting enzyme) and polymerase (RNA-synthesizing enzyme), respectively. ORF2 is expressed from a subgenomic RNA (shorter RNA segment) and encodes the VP90 capsid precursor protein (precursor of structural proteins).
Transmission and Epidemiology of Human Astrovirus
- Astroviruses are transmitted from person-to-person by the faecal–oral route (ingestion of contaminated material) or through contaminated food or water. Environmental transmission is supported by the stability of the virus in drinking water, freshwater, and marine water.
- Astrovirus is worldwide in distribution and tends to infect mainly children in the 1- to 3-year age group. Astroviruses have also been associated with foodborne outbreaks of gastroenteritis in Japanese adults and school children.
- They appear to account for 4 to 8.6% of all young children with diarrhea, depending on geographic location. Infections occur primarily in wintertime in temperate climates, similar to rotavirus.
- Astroviruses can cause sporadic outbreaks of diarrhea in elderly patients and are significantly associated with diarrheal illness in immunocompromised AIDS patients, solid organ transplant recipients, and bone marrow transplant recipients.
Replication of Human Astrovirus
- Attachment to host receptors (virus binds to cell surface proteins) probably mediates endocytosis (virus internalization into the cell).
- Uncoating, and release of the viral genomic RNA (virus genetic material) into the cytoplasm (intracellular fluid).
- The genome is then translated, giving rise to nsP1a1b and nsP1a polyproteins, which are cleaved by the viral serine protease (virus-encoded protein cutter) in nsP1a, as well as by some cellular proteases, resulting in the individual nonstructural proteins (viral proteins not part of capsid).
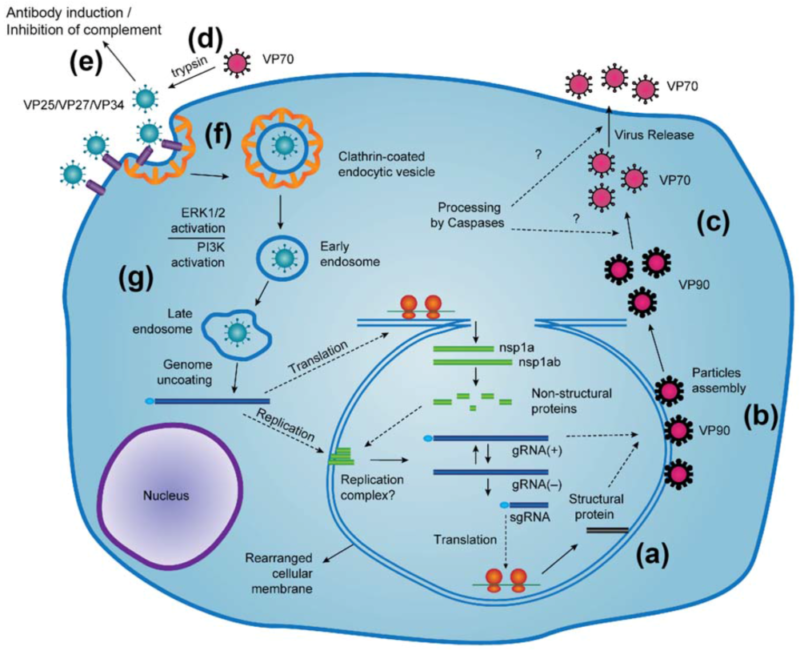
- Proteolytic processing of polyproteins nsP1a1b produces nsP1b protein (RdRp) (RNA-dependent RNA polymerase) and nsP1a protein, which is subsequently cleaved to yield several mature products.
- Replication occurs in viral factories (intracellular replication sites) made of membrane vesicles derived from the ER (endoplasmic reticulum).
- A full-length negative-sense genomic RNA (complementary RNA template) is synthesized and used as a template for the production of both positive-sense genomic RNA and positive-sense subgenomic RNA.
- Subgenomic RNA translation gives rise to the capsid protein precursor VP90 (initial capsid polyprotein).
- VP90 polyprotein initially assembles into immature virions (non-infectious viral particles) in association with intracellular membranes through its C terminus; several cellular caspases (host proteases) further cleave VP90 close to the C termini, resulting in viral capsids composed of VP70 (70-kDa polyproteins).
- Finally, VP70-containing viral particles are released from cells and proteolytically processed by trypsin (enzymatic cleavage to enhance infectivity).
- Virus release occurs by cell lysis (host cell rupture) and maturation of the capsid by proteolytic cleavages.
Pathogenesis of Human Astrovirus
- Spread may occur via the fecal–oral route (ingestion of contaminated material) from person-to-person contact or through contaminated food or water. Astrovirus pathogenesis (mechanism of causing disease) has not been well studied in humans.
- Viral particles have been visualized by EM (electron microscopy) in intestinal epithelial cells and in epithelial cells located in the lower part of the villi, suggesting the intestine is the primary site of replication, but systemic spread has been described in immunocompromised children.
- Astroviruses cause gastroenteritis by destruction of the intestinal epithelium, leading to inhibition of absorption, loss of secretory functions, and decreased epithelial permeability. Although mucosal IgA (secretory antibody in intestines) is induced upon HAstV infection, it is unclear whether it is required for protection.
- Intestinal biopsy specimens from healthy adults in an organ culture system with inactivated HAstVs demonstrated HAstV-specific CD4+ and CD8+ T cells (adaptive immune cells) residing in the tissue. Both humoral (antibody-mediated) and cellular adaptive immune responses are involved in protecting healthy adults from reinfections.
- Very high levels of virus (up to 10¹³ genome copies/g) can be present in stools, and virus excretion can be detected for up to two weeks after symptoms have cleared.
Clinical Manifestations of Human Astrovirus
Astrovirus gastroenteritis, seen mainly in young children, is usually mild. Mean incubation period is 4–5 days, followed by watery diarrhea lasting 1–4 days or more, along with abdominal discomfort, vomiting, fever, and anorexia (loss of appetite).
Vomiting is less common than in rotavirus or calicivirus infection, and the disease is usually milder. Children may shed virus 1–2 days prior to illness and for 4–5 days following illness. Children with poor nutritional status may develop more severe disease or chronic diarrhea.
Diagnosis of Human Astrovirus
- HAstVs are routinely detected by direct transmission electron microscopy (EM) in negatively stained stool samples.
- Cell culture propagation is possible for some classic HAstVs with trypsin, but virus isolation in culture is generally not applicable for diagnosis in fecal specimens.
- Enzyme immunoassay (antibody-based detection) using monoclonal antibody to group antigen to capture virus.
- Latex agglutination test specific for HAstV-1 serotype has been reported.
- ELISA and immunofluorescence methods detect serum antibodies.
- RT-PCR (reverse transcription polymerase chain reaction) has been used for genotyping human astroviruses.
Treatment of Human Astrovirus
No antiviral therapy is available. Supportive treatments include oral or intravenous fluid replacement to prevent dehydration.
Prevention and Control of Human Astrovirus
No vaccine is available. Control includes detection and inactivation of virus in water and food and disinfection of contaminated fomites (objects that may carry virus).