Coronaviruses
(enveloped RNA viruses) fall in the virus family Coronaviridae,
order Nidovirales.
They
are enveloped, 120–160 nm particles containing an unsegmented
genome of single-stranded positive-sense RNA (27–32 kb).
The
large plus-stranded RNA genome associates with the N protein
(nucleocapsid protein) to form a helical nucleocapsid, 9–11
nm in diameter.
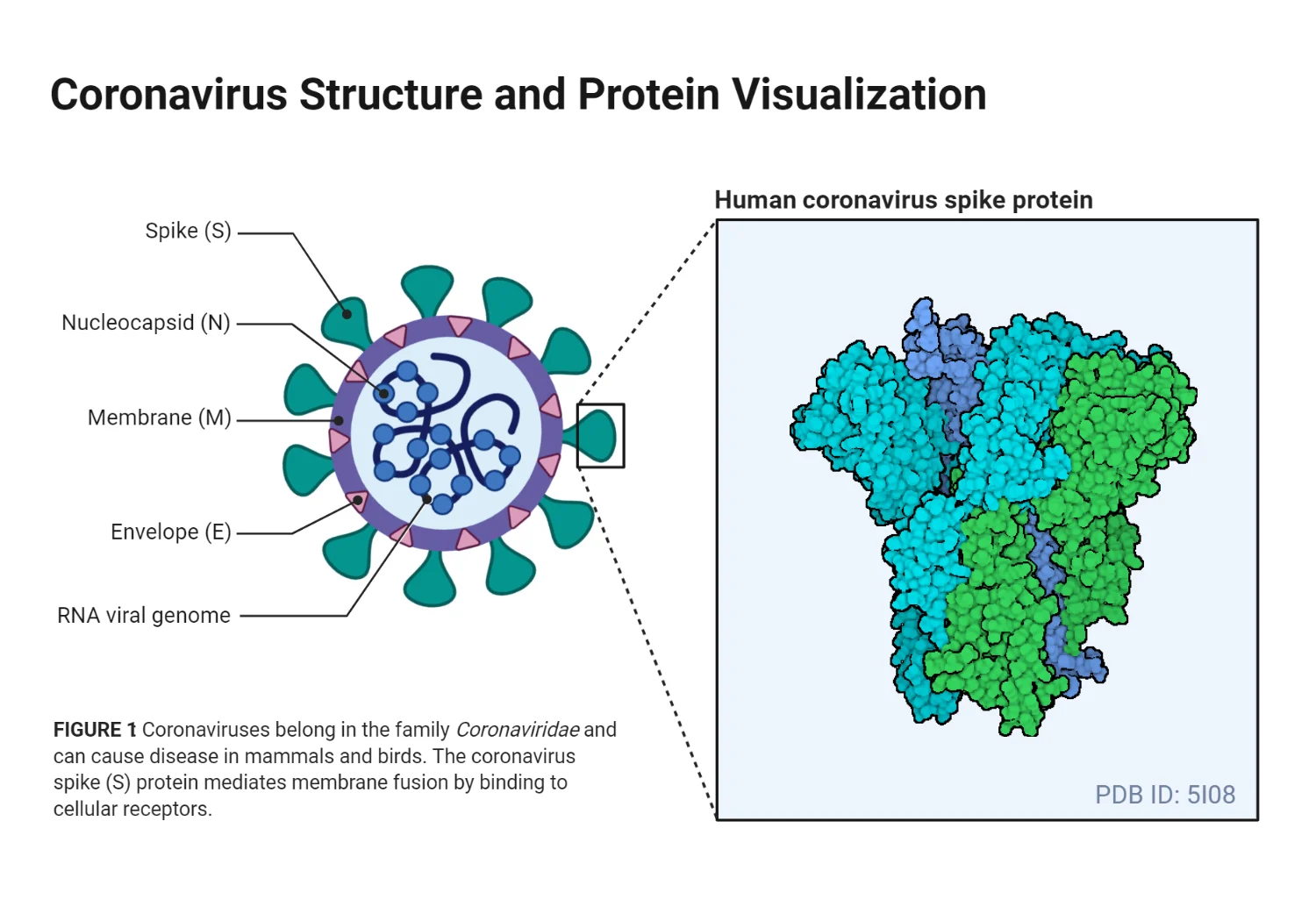
Spike
projections: 20 nm long, club- or petal-shaped, widely spaced on the
envelope, giving a “solar corona” appearance.
Viral
structural proteins:
Nucleocapsid
(N) protein (50–60 kDa, phosphorylated)
Membrane
(M) glycoprotein (20–35 kDa, matrix protein, interacts with
nucleocapsid)
Spike
(S) glycoprotein (180–220 kDa, forms petal-shaped peplomers)
Some
viruses (e.g., HCoV-OC43) also have HE glycoprotein (65
kDa) causing hemagglutination (clumping of red blood cells)
and possessing acetylesterase activity.
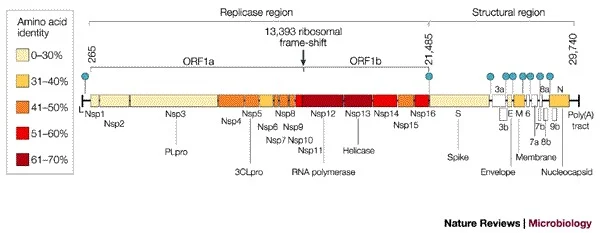
Genome of Coronavirus
Coronavirus
genomes are monopartite, single-stranded, positive-sense,
polyadenylated, and capped RNAs of 27–32 kb.
The 5′
end (~20–22 kb) carries the replicase gene, encoding multiple
enzymatic activities.
Replicase
gene products: encoded within ORFs 1a and 1b (open reading
frames).
Order
of structural genes: Pol-S-E-M-N (Polymerase, Spike, Envelope,
Membrane, Nucleocapsid).
Additional
ORFs encode 2–4 nonstructural proteins of unknown function.
Intergenic
sequence (IS): ~7 bases at the 5′ end of each gene, essential for subgenomic
RNA formation.
Infected
cells contain overlapping subgenomic, capped, and polyadenylated mRNAs.
Each
subgenomic mRNA and genomic RNA is translated to produce only the
protein encoded by the 5′ gene.
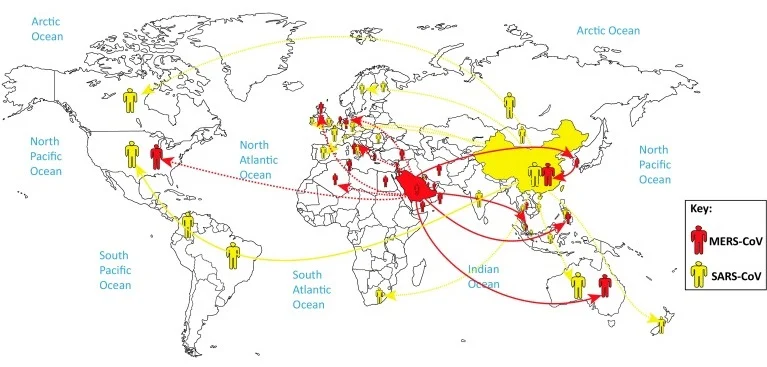
Epidemiology of Coronavirus
Natural
outbreaks of coronavirus-caused colds occur mostly in winter.
Coronaviruses
cause 15–30% of all colds.
HCoV 229E,
OC43, NL63 are found worldwide.
Contribution
of each HCoV varies yearly: e.g., 229E can account for 1%–35% of acute
respiratory infections.
Incidence
fluctuates: one 3-year study showed 1%–35% infection rates.
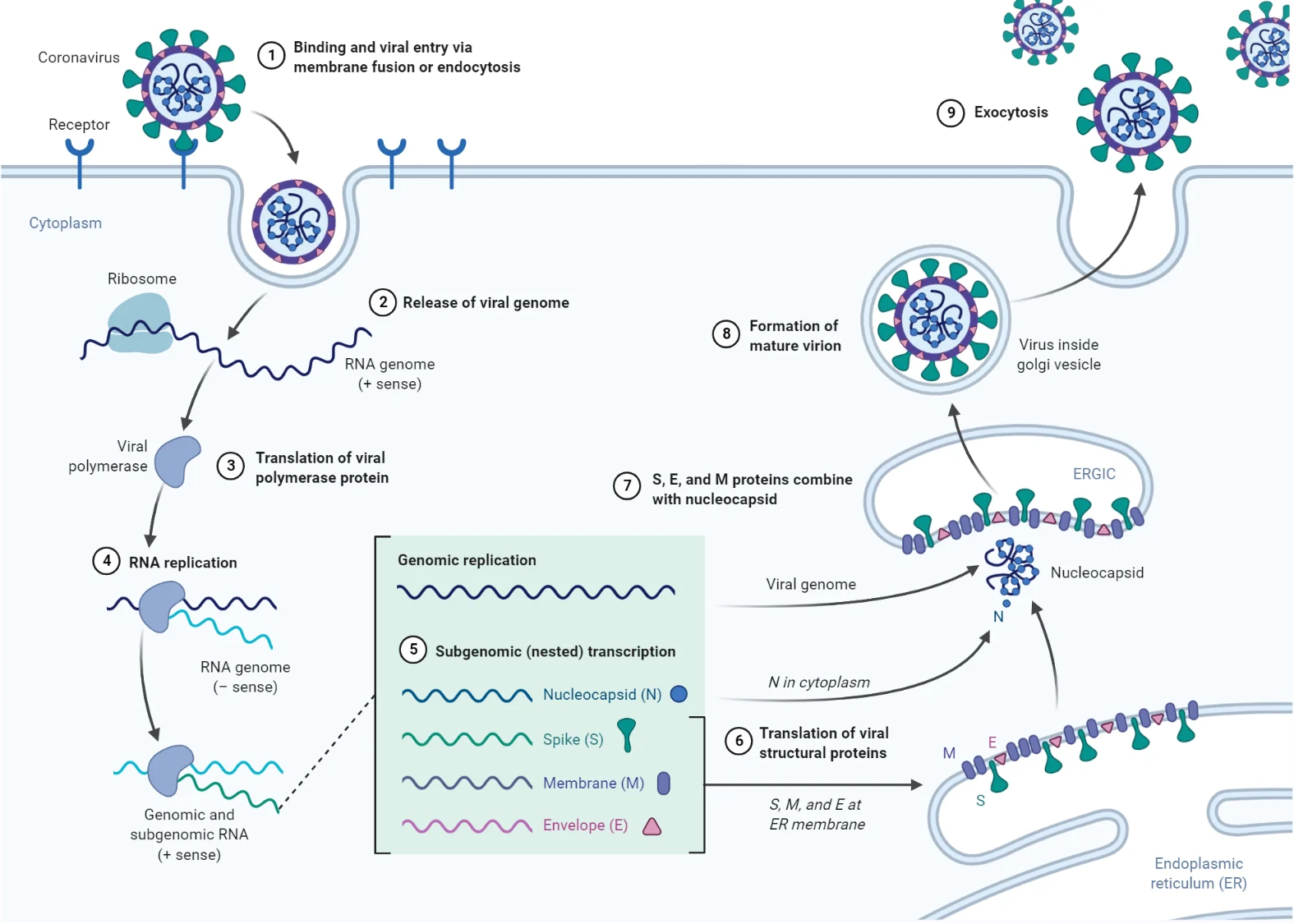
Replication of Coronavirus
Human
infection occurs via respiratory secretions.
Attachment:
mediated by S glycoproteins binding to host cell receptors.
Entry:
fusion of viral envelope with host membrane or receptor-mediated
endocytosis.
229E
and NL63 bind aminopeptidase N and ACE-2, respectively.
Receptors
for OC43 and HKU-1 are unknown.
Fusion:
mediated by S2 portion of spike protein (class 1 fusion protein).
Translation
of genomic RNA → large polyprotein → processed into RNA-dependent
RNA polymerase (RdRp).
RdRp
synthesizes a negative-strand RNA, template for nested set of
subgenomic mRNAs.
Translation
of subgenomic mRNAs → structural proteins.
N
protein + genomic RNA → helical nucleocapsids.
Membrane
glycoprotein M: inserted into ER, anchored in Golgi
apparatus.
Nucleocapsid
+ M protein assemble at budding compartment (ERGIC).
E
and M proteins trigger virion budding, enclosing nucleocapsid.
Pathogenesis of Coronavirus
Primary
route of transmission: via the respiratory tract, spread by aerosols
and large droplets (e.g., sneezes).
Infection
with common-cold coronaviruses causes ciliostasis (loss
of ciliary action) and degenerative changes in respiratory
epithelial cilia.
Infection
is usually localized to the upper respiratory tract because the
optimum viral growth temperature is 33–35°C, though it may extend
to the lower respiratory tract in some cases.
HCoV-OC43
generally causes mild upper respiratory infections, but may exhibit
neuroinvasive properties.
Clinical Manifestations of Coronavirus
HCoVs
in the 229E- and OC43-related serogroups cause upper respiratory
symptoms in adults and children, varying in frequency and severity.
Respiratory
infections include bronchiolitis and pneumonia; gastroenteritis
and neurological disorders can also occur.
In
adults, HCoVs usually cause “common colds”, often afebrile.
I’m an accidental blogger and a microbiologist by education. I have dedicated my past 5+ years of learning to the field of life science. helping numerous individuals and providing useful educational ......